Hello, everyone!
Here are some home health-related updates for this week:
AMITY’S NEWS
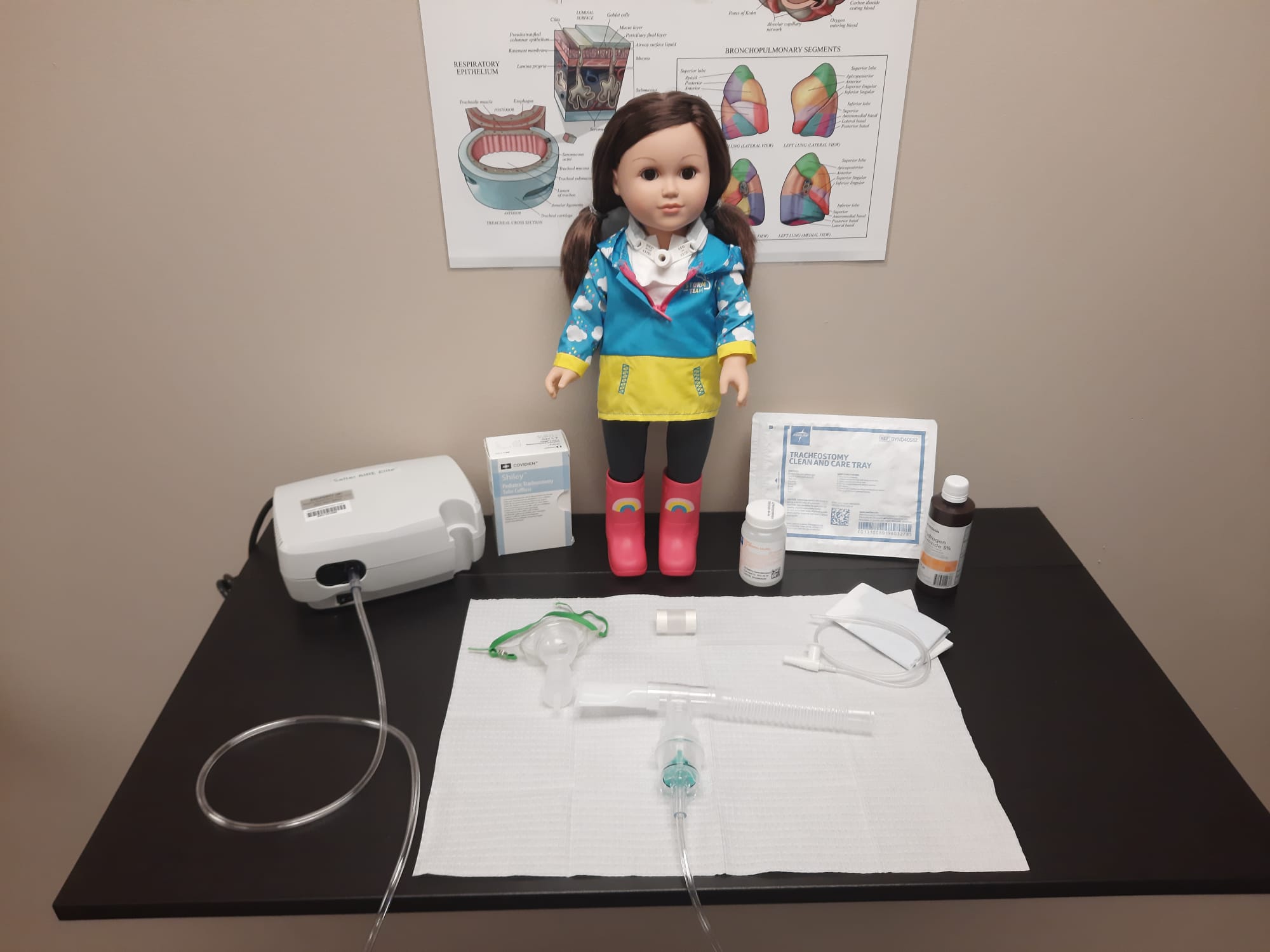
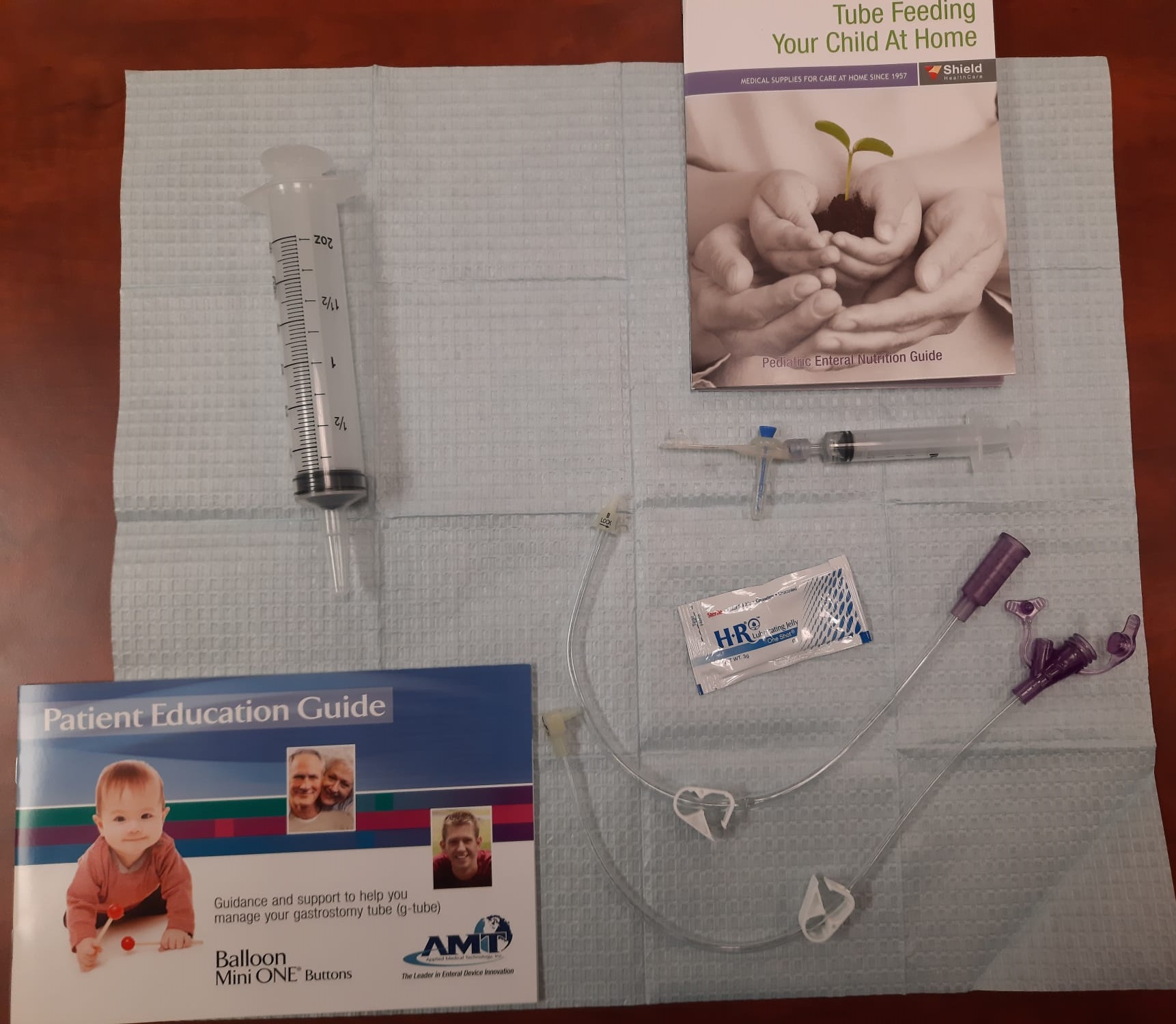
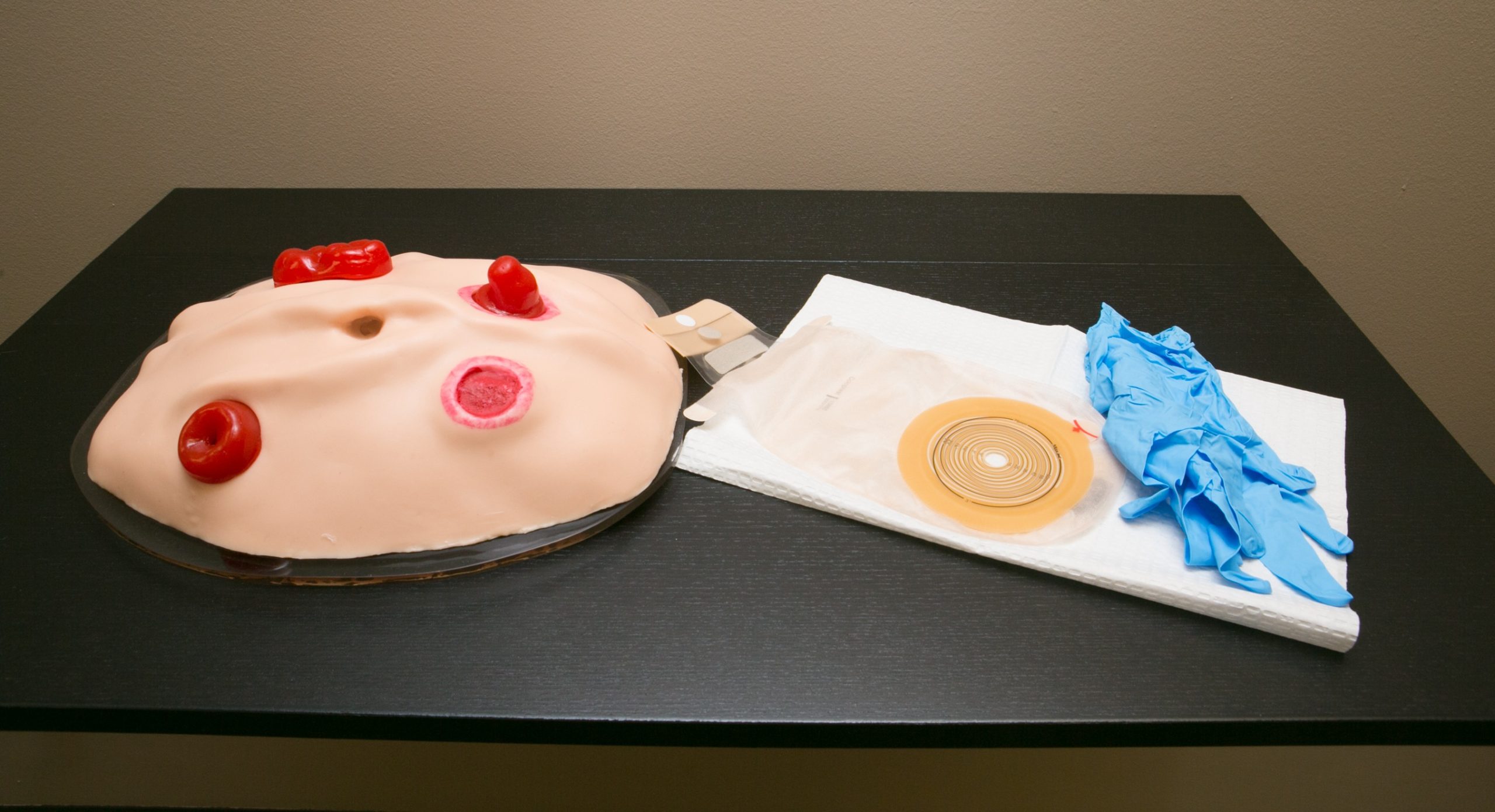
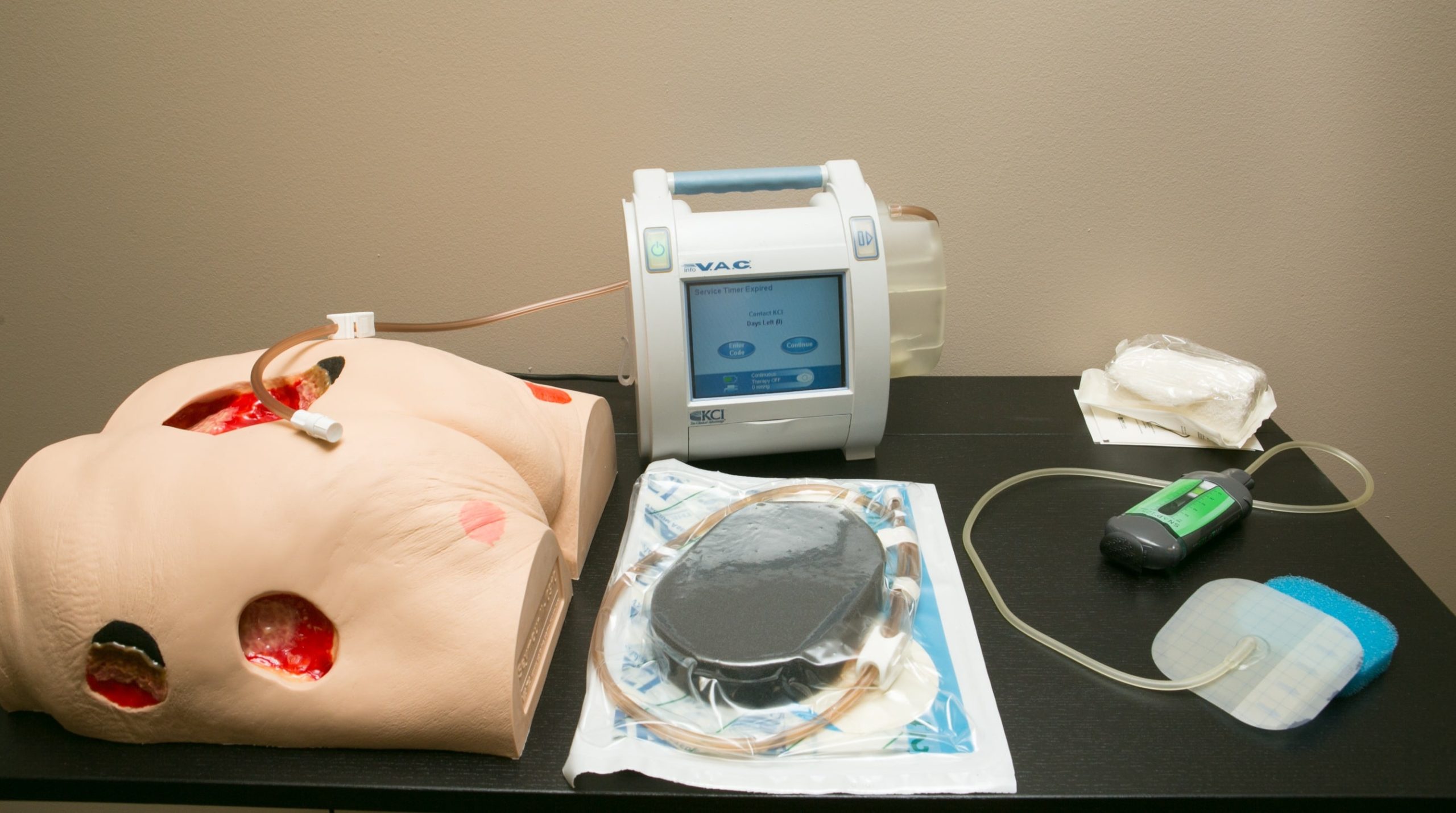
OUR VIRTUAL SKILLED NURSING COMPETENCY PROGRAM IS OFF TO A GREAT START!
We have been getting very positive feedback from the participants.
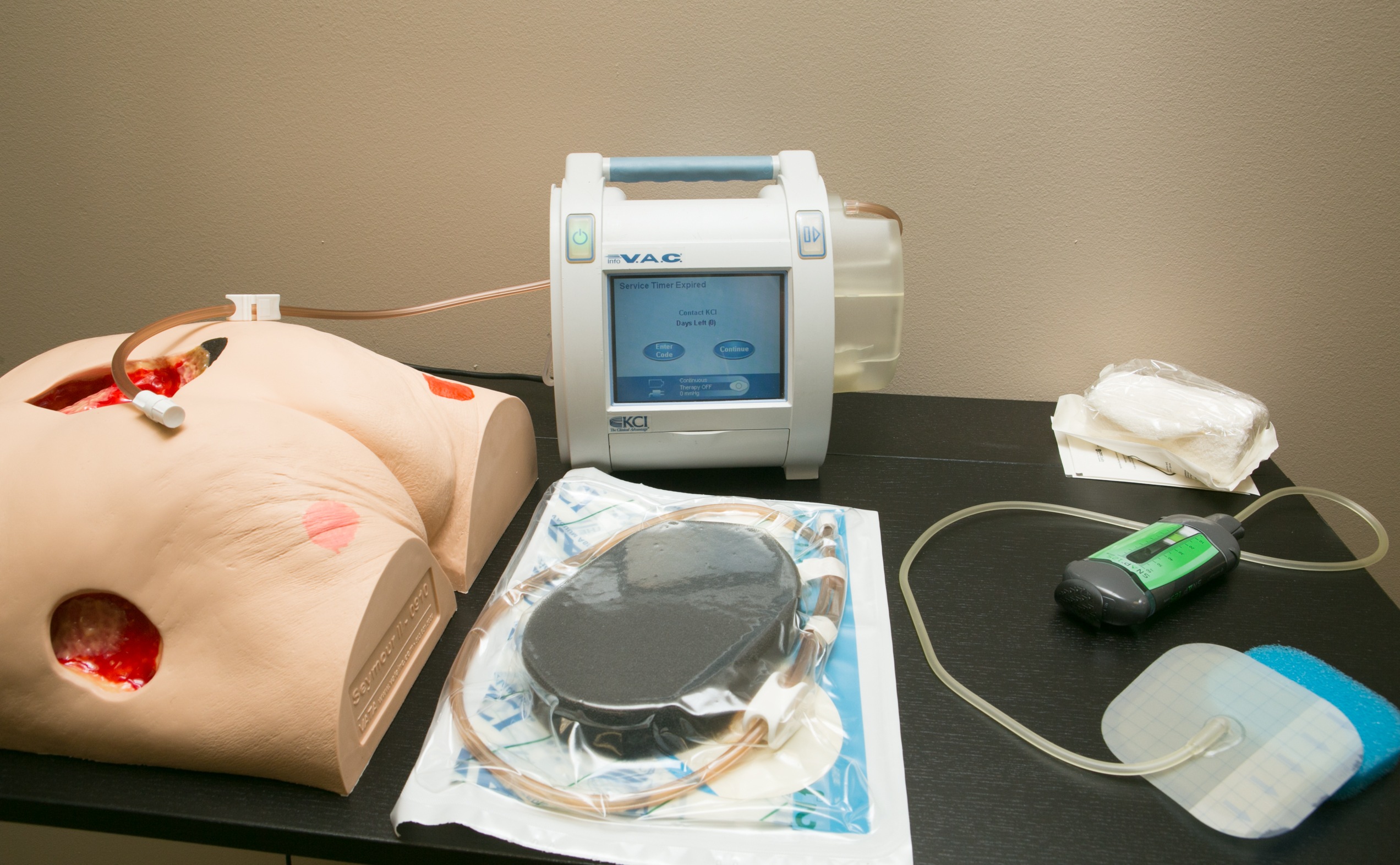
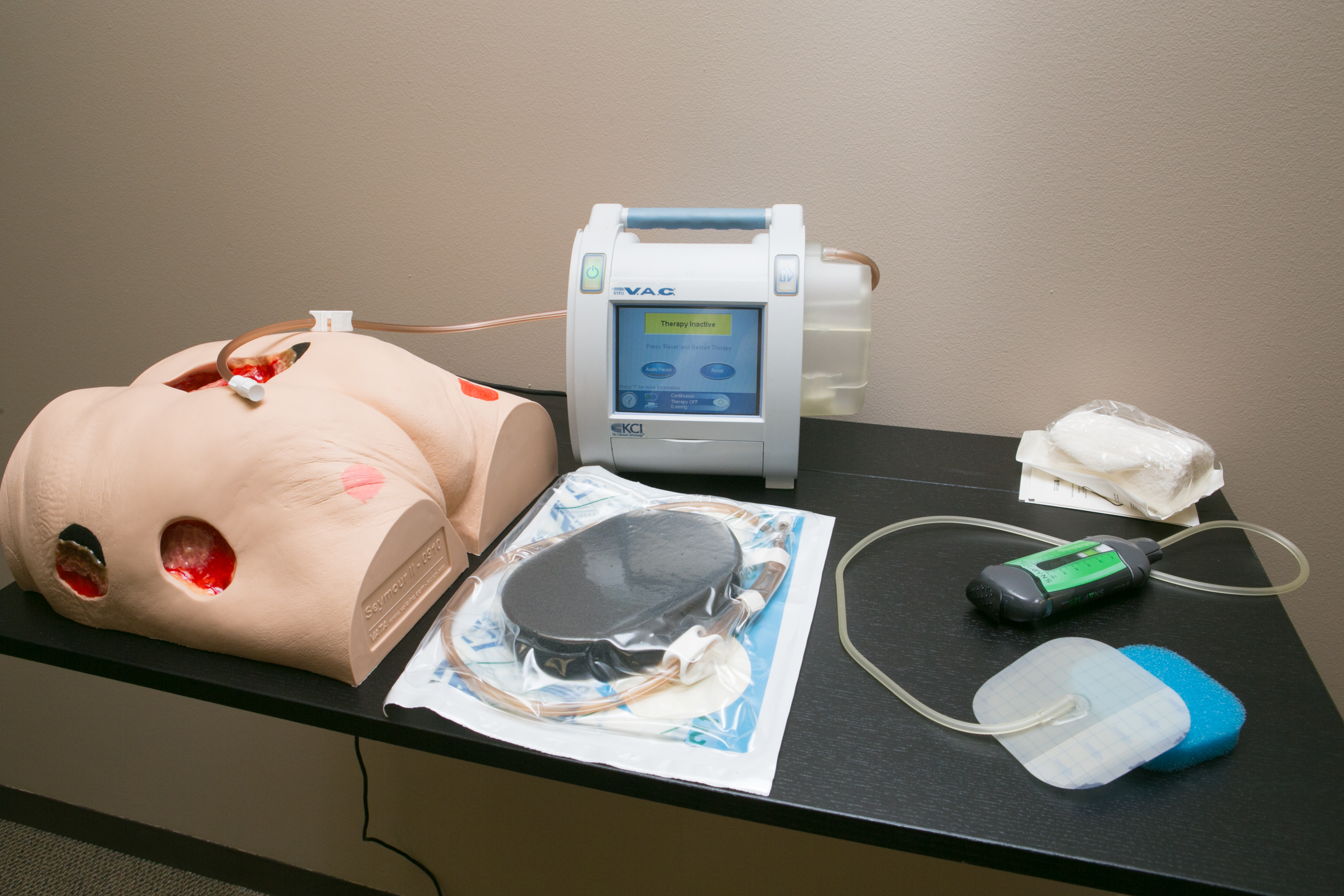
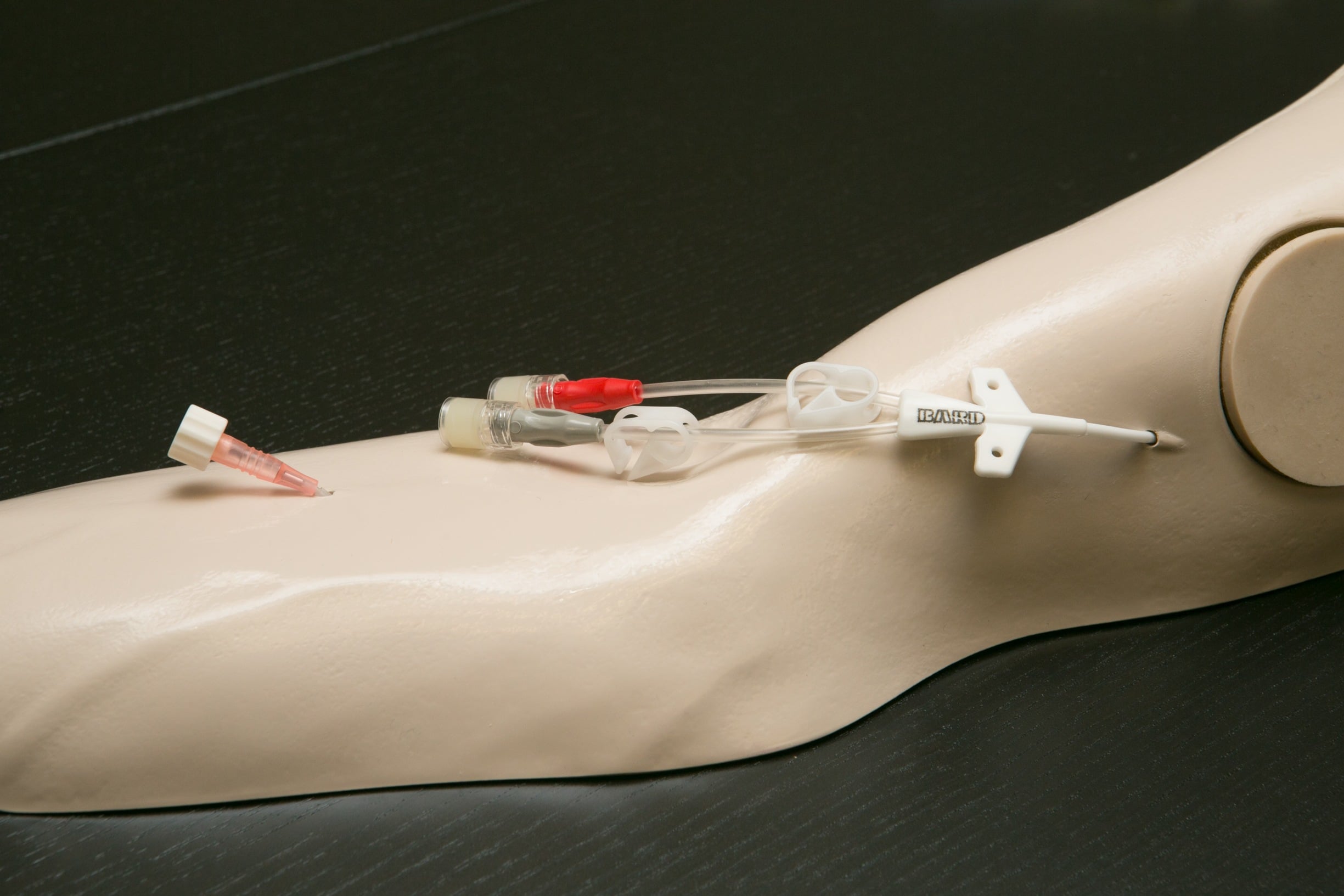
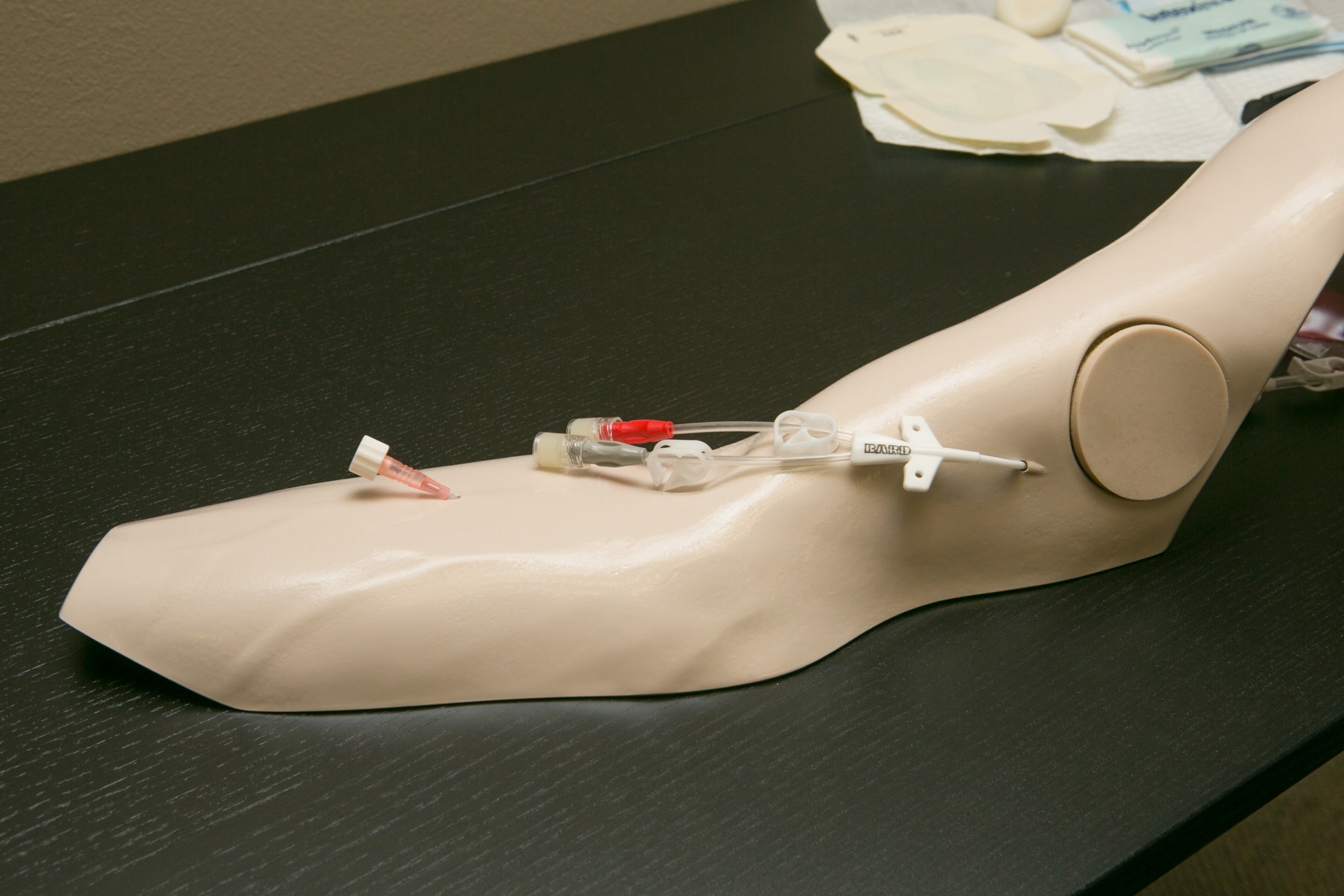
“This was a great class. The lecture/videos were relevant, detailed and were very useful. I have been a home health RN for many years and this was a great review/refresher and provided a ton of useful information. I think it was adequate for nurses new to home health as well. The instructors were engaged and worked to make the content personal and I felt that they were trying to connect with the students. The written test provided a good assessment of knowledge. I especially loved the practicum portion and that I could demonstrate the skills with actual tools. This program was a wonderful experience and I recommended that my company use this for the rest of my nursing team.“
To register for a virtual skilled nursing competency, please go to: https://amityhealthcaregroup.com/virtual-nursing-competency/
Please call 303-690-2749 for additional questions.
NATIONAL NEWS
Home Health Payment Corrections
Medicare announced that as of April 1, 2021, Medicare systems corrected 3 errors affecting the payment of Calendar Year (CY) 2021 claims:
-
- Claims spanning January 1 are applying CY 2020 rates in error
- Late Request for Anticipated Payment (RAP) penalties are not applying to outlier amounts
- Late RAP penalties are being applied after the Value-Based Purchasing (VBP) adjustment when the VBP adjustment should be the last calculation
Accelerated and Advance Payment Recoupment to Begin
For the providers who received funds from accelerated and advance payment loans, please note that CMS will begin to recoup any outstanding balance from any payments due from your Medicare claims. The recoupment started as of March 30, 2021. The recoupment date will depend upon the 1-year anniversary of when you received your first payment.
Recoupment rate: For the first 11 months of the repayment period, the recoupment rate will be 25% of the claims due to the provider or supplier. During the last six months, the offset will be 50% of the claims due to the provider.
Repayment period: The repayment timeline before interest starts to accrue on the loan is effectively 29 months.
Interest rate: If a loan is not fully paid off during the 29- month repayment period, CMS starts to charge interest on the loan. That interest rate is 4%
For a special edition of the MLN Matters Article for Medicare providers and suppliers who requested and received COVID-19 Accelerated and Advance Payments, please go to https://www.cms.gov/files/document/se21004.pdf
Extension of Medicare Sequestration Moratorium
As you know, the Medicare Sequestration moratorium was set to expire on 3/31/2021. However, the Senate passed a Bill that extends the moratorium through 12/31/21. The next step is for the House of Representatives to act on the Senate’s Bill after their return to session on 04/13/21 or earlier by proxy vote.
As the result, CMS issued the following notification for Medicare providers and suppliers on March 30, 2021:
Temporary Claims Hold Pending Congressional Action to Extend 2% Sequester Reduction Suspension
In anticipation of possible Congressional action to extend the 2% sequester reduction suspension, we instructed the Medicare Administrative Contractors (MACs) to hold all claims with dates of service on or after April 1, 2021, for a short period without affecting providers’ cash flow. This will minimize the volume of claims the MACs must reprocess if Congress extends the suspension; the MACs will automatically reprocess any claims paid with the reduction applied if necessary.
New Provider Enrollment Administrative Action Authorities
On March 24, 2021, CMS released information about recently issued regulatory authorities that may affect currently enrolled Medicare providers and suppliers, or prospective providers and suppliers.
As the result of the above, Medicare will require affiliation disclosures from all providers and suppliers on all initial and revalidation Medicare enrollment applications.
Reporting Requirement
Upon a CMS request, providers or suppliers initially enrolling or revalidating will be expected to disclose any and all affiliations that it or any of its owning or managing employees or organizations has had within the previous 5 years with a currently or formerly enrolled Medicare, Medicaid, or CHIP provider or supplier that has a disclosable event.
Types of Affiliations
The following roles create affiliations that may lead to a determination of the undue risk of fraud, waste, or abuse when coupled with a disclosable event (see below):
- A 5-percent or greater direct or indirect ownership interest that an individual or entity has in another organization
- A general or limited partnership interest (regardless of the percentage) that an individual or entity has in another organization
- An interest in which an individual or entity exercises operational or managerial control over, or directly or indirectly conducts, the day-to-day operations of another organization (including, for the purposes of the affiliation requirement only, sole proprietorships), either under contract or through some other arrangement, regardless of whether or not the managing individual or entity is a W-2 employee of the organization
- An interest in which an individual is acting as an officer or director of a corporation
- Any reassignment relationship under 42 Code of Federal Regulations (CFR) Section 424.80
Per CMS, “we will not request affiliation disclosures until we revise the Form CMS-855 applications with affiliation disclosure sections. This includes online enrolment applications in the Provider Enrollment Chain and Ownership System (PECOS). Note: In light of the pandemic and various other factors, we will not begin updating the Form CMS-855 applications with affiliation disclosure sections for at least another 12 months.”
For a complete copy of the special edition of the MLN Matters Article, please go to: https://www.cms.gov/files/document/se21003.pdf
CMS Issues Update to Emergency Preparedness Guidance/Appendix Z
On March 26, 2021, CMS has updated its interpretive guidance on emergency preparedness, Appendix Z of the State Operations Manual. Most of these changes to the interpretive guidance reflect regulatory changes that were made in 2019 as follows:
- The Burden Reduction Final Rulechanged the frequency of updates required for non-long term care providers and changes to the training and testing program.
- CMS added “emerging infectious diseases” (or “EIDs”) to the definition of all-hazards approaching Appendix Z so health facilities would include planning for infectious diseases within their emergency preparedness program. In addition, as the result of the COVID-19 Public Health Emergency, CMS expanded the interpretive guidelines to include best practices, lessons learned, and planning considerations for emerging infectious diseases.
For a complete CMS “Updated Guidance for Emergency Preparedness-Appendix Z of the State Operations Manual (SOM) ”memo, please go to:
https://drive.google.com/file/d/19i4_4T-gtGNatK0LNExyFmKncN64pXYE/view
CDC Updates for Fully Vaccinated Health Care Personnel
In March, CDC issued additional guidelines for fully vaccinated health care personnel as follows (please update your protocols accordingly):
- Fully Vaccinated HCP with higher-risk exposures who are asymptomatic no longer need to be restricted from work for 14 days following their exposure.
- HCP who have recovered from SARS-CoV-2 infection in the prior 3 months of a higher-risk exposure are also no longer required to quarantine if they remain asymptomatic.
- NOTE: HCP who have underlying immunocompromising conditions (e.g., organ transplantation, cancer treatment) which may impact the level of protection provided by the COVID-19 vaccine should continue to implement work restrictions if they have incurred a higher risk exposure.
- Fully Vaccinated HCP who have traveled should continue to follow the same CDC recommendation
as recommended for any traveler. This includes the following:
o Get tested with a viral test 3-5 days after travel and stay home and self-quarantine for a full 7 days after travel.
▪ Even if you test negative, stay home and self-quarantine for the full 7 days.
▪ If you test positive, isolate yourself to protect others from getting infected.
o If you do not get tested, stay home and self-quarantine for 10 days after travel.
o Avoid being around people who are at increased risk for severe illness for 14 days.
- Recommendations for testing of HCP remain unchanged, whether fully vaccinated or not.
o Four situations may require testing.
▪ Testing of HCP with signs and symptoms consistent with COVID-19 is a priority.
- Even a sore throat may be possible consideration for testing due to the extensive and close contact of HCP with vulnerable populations.
▪ Testing asymptomatic HCP with known high-risk exposure may be a priority also due to the contact with vulnerable populations. The CDC recommends HCP err on the conservative side.
▪ Testing of asymptomatic HCP without known or suspected exposure is primarily completed as part of expanded screening in skilled facilities
▪ Testing of HCP may be done of those diagnosed with infection to determine that they are no longer infectious although a symptom-based method may actually result in less quarantine time due to the potential viral load causing continuing positive results.
- PPE usage remains unchanged for HCP who are fully vaccinated.
COLORADO NEWS
Colorado Medicaid Home Health and Private Duty Nursing Rate Increase Approved
On April 1, 2021 Home Care and Hospice Association of Colorado announced the following:
“In a last-minute motion, prior to finalizing the budget package, the Joint Budget Committee (JBC) approved a targeted increase of $7 million to be split evenly between skilled home health and private duty nursing rates. This increase is in addition to the 2.5% “across the board” provider rate increase that was approved. The introduced FY2021-22 Long Bill will contain the following increases:”
Home Health: +7.3% (brings Medicaid from 73% to 80% of LUPA rates)
PDN – LPN: +10.5%
PDN – RN: +5.6%
Note: more information on the effective dates and rate schedule is to come.
Thank you to HHAC and the Legislators who support home health industry!
Healthcare Facility Visitor Screening and Triage for Signs and Symptoms of COVID-19:
Just a note and a reminder that the memo below was issued by CDPHE in the Fall of 2020. Per coordination with CPDHE on April 1, 2021, this memo remains to be in effect and it does apply to Home Health Agencies “as they are required to have an office where staff and patients could potentially enter.” Please assure that you have appropriate procedures in place.
To: Owners, Administrators, Directors, Risk Management
From: HFEMSD
Based on the Center for Disease Control (CDC) summary of changes to the guidance for: Interim Infection Prevention and Control Recommendations for Healthcare Personnel During the Coronavirus Disease 2019 (COVID-19) Pandemic, the following revised screening steps are required for ALL licensed facilities.
Screen and Triage Everyone Entering a Healthcare Facility for Signs and Symptoms of COVID-19:
Establish a process to ensure everyone (patients, healthcare personnel, and visitors) entering the facility is assessed for symptoms of COVID-19, or exposure to others with suspected or confirmed SARS-CoV-2 infection and that they are practicing source control.
- Options could include (but are not limited to): individual screening on arrival at the facility; or implementing an electronic monitoring system in which, prior to arrival at the facility, people report absence of fever and symptoms of COVID-19, absence of a diagnosis of SARS-CoV-2 infection in the prior 10 days, and confirm they have not been exposed to others with SARS-CoV-2 infection during the prior 14 days.
- Fever can be either measured temperature ≥100.0°F or subjective fever. People might not notice symptoms of fever at the lower temperature threshold that is used for those entering a healthcare setting, so they should be encouraged to actively take their temperature at home or have their temperature taken upon arrival.
Amity’s Friday emails (newsletters) will be archived on Amity’s Healthcare Group website at https://amityhealthcaregroup.com/resources/ under Weekly Newsletter section.
PLEASE NOTE THAT EFFECTIVE MARCH 19, 2021, AMITY HEALTHCARE GROUP WILL BE PUBLISHING ITS NEWLETTER BI-WEEKLY.
Please do not hesitate to reach out for any assistance or questions via email, phone or website at https://amityhealthcaregroup.com/resources/
If you wish to forward this email to your colleague or friend, please feel free to do so. If you received this message as a forward, we invite you to subscribe to our communications at https://amityhealthcaregroup.com/ (look for “Subscribe to Listserv” in the top corner). If you wish to unsubscribe from this email distribution list, please email to eg@amityhealthcaregroup.com
Thank you,
Irina Gorovaya, RN BSN, MBA
Amity Healthcare Group, LLC
Home Health Consulting, Education and Outsourcing Services
720-353-7249 (cell) 303-690-2749 (office) 720-398-6200 (fax)




























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}