Amity’s News!
Amity Healthcare Group Home Health Policy and Procedure Manual Received ACHC Certification.
ACHC certification is a verification that the product is in compliance with ACHC requirements.
![]()
Our Policy and Procedure Manual has been designed to meet ACHC standards and Medicare Conditions of Participation for home health organizations. The manual is customizable to further meet your agency needs and align the proposed policies and procedures with the internal organizational practices while ensuring compliance with Medicare Conditions of Participation and ACHC standards. The manual also includes multiple forms, practical tools, and references. State-specific Policy and Procedure manuals are available upon request.
For more information, please go to https://amityhealthcaregroup.

Other ACHC Certified Products:-
- Home Health and Home Care admission packet
- Home Health QAPI program and Home Care PI program
- Home Health and Home Care Emergency Preparedness Plan
- Home Health Skilled Nursing Competency Program
ORDER YOUR COPY TODAY
For more information about our ACHC certified products, please call 303-690-2749 or email ig@amityhealthcaregroup.com.
Please also visit our website at https://amityhealthcaregroup.
OASIS -E Corner

In this newsletter, we would like to discuss section GG- Functional Abilities and Goals.
![]()
The time period to consider for coding this item is “Day of Assessment” which is defined as the 24 hours that immediately precedes the assessment and the time spent by the clinician conducting the assessment.
OASIS Guidance Manual Response Specific Instructions:
- Licensed clinicians may assess the patient’s self-care and mobility performance based on:
- direct observation (preferred),
- patient/caregiver report,
- assessment of similar activities and/or
- collaboration with other agency staff who have had direct contact with the patient or some other means of gathering information.
- If the patient only completes a portion of the activity (e.g., performs a partial bath or transfers into but not out of a vehicle) and does not complete the entire activity during the assessment timeframe, use clinical judgment to determine if the situation allows the clinician to adequately assess the patient’s ability to complete the activity. If the clinician determines that this observation is adequate, code based on the type and amount of assistance the patient requires to complete the ENTIRE activity. If the clinician determines the partial activity does not provide adequate information to support determination of a performance code, select an appropriate “activity not attempted” code.
- When a GG function activity is not completed entirely during one clinical observation (i.e., a patient transfers bed-to-chair in the morning, and transfers chair-to-bed at night), code based on the type and amount of assistance required to complete the ENTIRE activity.
- Patients should be allowed to perform activities as independently as possible, as long as they are safe.
- When using patient or caregiver reports, it is expected that the patient and caregivers are reporting on the patient’s status within the time period under consideration (e.g., reporting on the patient’s ability to complete an activity within the past 24 hours).
- For GG0130 and GG0170 the assessing clinician would code each activity based on the type and amount of assistance needed to complete the activity safely, not based on the availability of such assistance.
Tips: First see if codes 01-06 apply. Activity not attempted codes would not apply if the caregiver does the task completely for the patient.
NATIONAL NEWS

CMS Proposed CY2024 Home Health Rule
July brought forth a highly anticipated unveiling of the proposed CY2024 Home Health Rule.
![]()
In addition to rate updates for home health agencies, the rule includes proposals to revise the Home Health Quality Reporting Program (HHQRP), the Home Health Value Based Purchasing (HHVBP) demonstration project, and claims processing for disposable negative pressure wound therapy (dNWPT). The rule also includes two requests for information (RFIs): Access to Home Care Services and Principles for Selecting and Prioritizing HH QRP Quality Measures and Concepts.
The proposed rule can be downloaded from the Federal Register at: https://www.federalregister.
Below, you will find some of the details of the proposed CY2024 Home Health Rule as provided by the National Association for Home Care and Hospice (NAHC):
Rates Update:
- A net 2.7% inflation update (3.0% Market Basket Index – 0.3% Productivity Adjustment
- A -5.653% Budget Neutrality permanent adjustment to account for the remaining 3.925% adjustment from CY2023 plus the additional 2022 adjustment of 1.636%.
- Recalibration of the 432 case mix weights as CMS has done multiple times in recent years. The recalibration leads to a separate budget neutrality adjustment in the payment rates of 1.21%.
- CMS estimates that Medicare payments to HHAs in CY 2024 would decrease in the aggregate by 2.2 %, or $375 million compared to CY 2023, based on the proposed policies.
- The outcome of these payment rate changes on 30-day period base rates and per-visit LUPA rates is as follows. HHAs that failed to provide required quality data have these rates reduced by two percent.


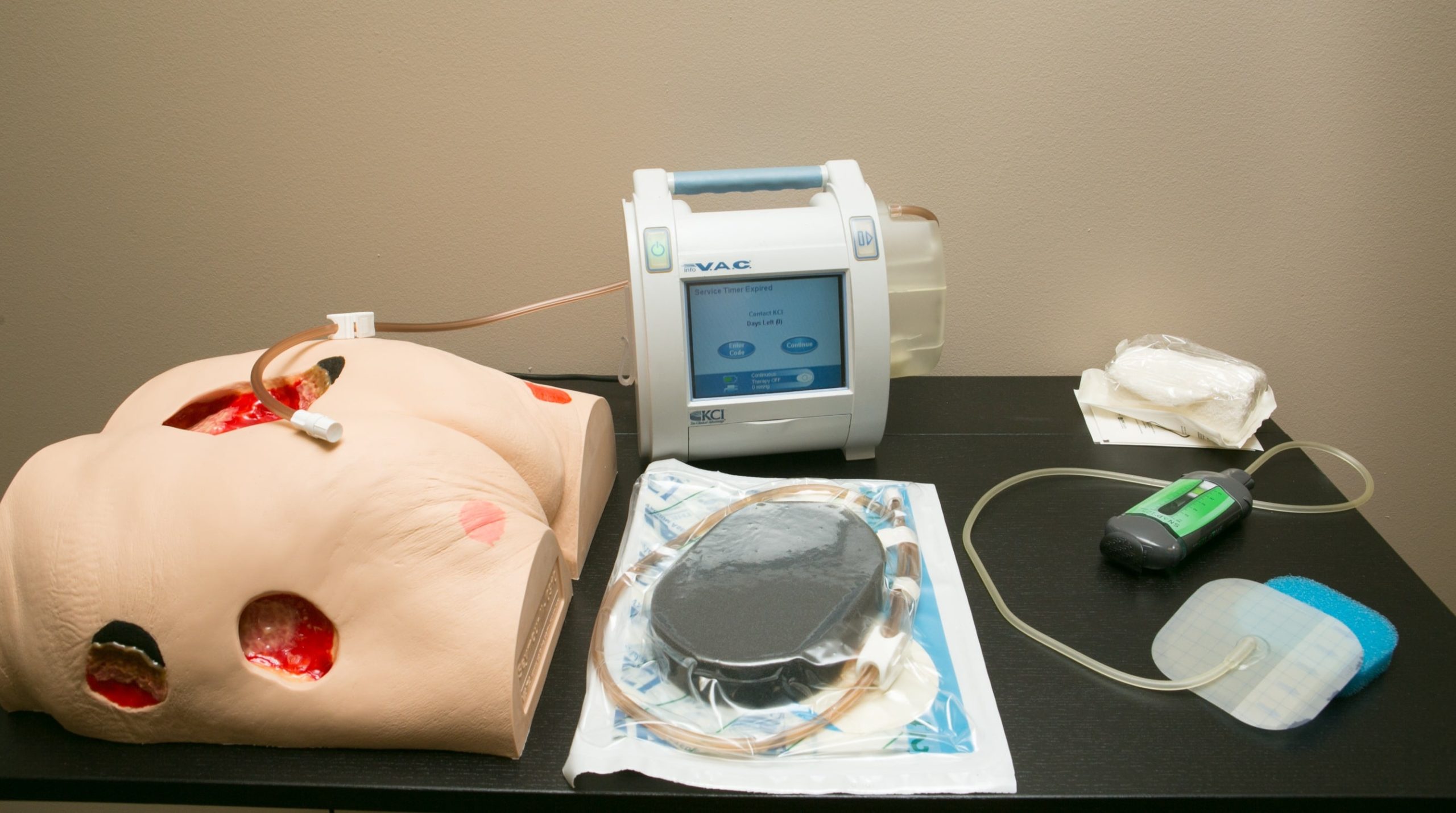
Disposable Negative Pressure Wound Therapy (dNPWT)
The Consolidated Appropriations Act, (CAA) 2023 included technical amendments for the payment of dNPWT. The Act modifies the methods for calculating separate payments for dNPWT devices for each of the next three years. Additionally, beginning January 1, 2024, payment for the device will be made separately from the nursing and therapy services associated with furnishing the device. Nursing and therapy visits provided for dNPWT will be billed separately on the home health claim type of bill (TOB) 32x. Beginning in calendar year (CY) 2024 and each subsequent year, claims for the separate payment amount of an applicable dNPWT device using Healthcare Common Procedure Coding System (HCPCS) code A9272 would be reported on claims submitted using the TOB 32x. That is, claims with a date of service on or after January 1, 2024 for an applicable dNPWT device will no longer be submitted on TOB 34X.
Home Health Value Based Purchasing Program (HHVBP)
For the expanded HHVBP Model, CMS is proposing to:
- Replace the two Total Normalized Composite Measures (for Self-Care and Mobility) with the Discharge Function Score measure effective January 1, 2025;
- Replace the OASIS-based Discharge to Community (DTC) measure with the claims-based Discharge to Community-Post Acute Care (PAC) Measure for Home Health Agencies effective, January 1, 2025;
- Replace the claims-based Acute Care Hospitalization During the First 60 Days of Home Health Use and the Emergency Department Use without Hospitalization During the First 60 Days of Home Health measures with the claims-based the Potentially Preventable Hospitalization measure effective January 1, 2025;
- Change the weights of individual measures due to the change in the total number of measures; and,
- Beginning with performance year CY 2025, CMS proposes to update the Model baseline year to CY 2023 for all applicable measures in the proposed measure set, including those measures included in the current measure set with the exception of the 2-year DTC-PAC measure, which would be CY 2022 and CY 2023.
Home Health Quality Reporting Program (HHQRP)
CMS is proposing the adoption of the following measures:
- COVID-19 Vaccine: Percent of Patients/Residents Who Are Up to Date (Patient/Resident COVID-19 Vaccine) measure to the HH QRP beginning with the CY 2025 HH QRP.
- CMS also proposes to adopt the Functional Discharge Score (DC Function) measure to the HH QRP beginning with the CY 2025 HH QRP.
CMS is proposing the removal of the following measures:
- With the addition of the Discharge Function measure, we propose to remove the Application of Percent of Long-Term Care Hospital (LTCH) Patients with an Admission and Discharge Functional Assessment and a Care Plan That Addresses Function (Application of Functional Assessment/Care Plan) measure from the HH QRP beginning with the CY 2025 HH QRP.
- Additionally, CMS is proposing removal of two OASIS items no longer necessary for collection, the M0110 – Episode Timing and M2220- Therapy Needs items.
CMS is proposing the public reporting of four measures:
- Discharge Function;
- Transfer of Health (TOH) Information to the Provider—Post-Acute Care (PAC) Measure (TOH-Provider);
- Transfer of Health (TOH) Information to the Patient—Post-Acute Care (PAC); and
- COVID-19 Vaccine: Percent of Patients/Residents Who Are Up to Date.
Proposed Changes to the Provider and Supplier Enrollment Requirements:
In response to program integrity concerns related to hospice and other providers, CMS is proposing several changes to existing Medicare provider enrollment regulations. They include:
Provisional Period of Enhanced Oversight: The HHS Secretary has authority to provide for a provisional period of between 30 days and 1 year during which new providers and suppliers would be subject to enhanced oversight (so-called Provisional Period of Enhanced Oversight – PPEO). This oversight can include prepayment review and payment caps, among other actions. In the rule CMS is proposing regulations under which a “new” provider would be defined as any of the following:
- A newly-enrolling Medicare provider or supplier (this includes providers that must enroll as a new provider in accordance with the change in majority ownership provisions in Section 424.550(b)).
- A certified provider or certified supplier undergoing a change of ownership consistent with the principles of 42 CFR 489.18 (including providers that qualify under Section 424.550(b)(2) for an exception from the change in majority ownership requirements in Section 424.550(b)(1) but which are undergoing a change of ownership under 42 CFR 489.18).
- A provider or supplier (including an HHA or hospice) undergoing a 100 percent change of ownership via a change of information request under Section 424.516.
CMS is proposing that the effective date of the PPEO’s commencement is the date on which the new provider or supplier submits its first claim (rather than, for example, the date the first service was performed or the effective date of the ownership change).
Retroactive Provider Agreement Termination: Under current policy, a provider may voluntarily terminate its provider agreement with Medicare and may do so on a retroactive basis. CMS is proposing to incorporate into regulation that a provider may request a retroactive termination date, but only if no Medicare beneficiary received services from the facility on or after the requested termination date.
Other Provider Enrollment Provisions:
To further protect the Trust Funds and Medicare beneficiaries, CMS is proposing additional provider enrollment provisions, which include, but are not limited to, the following:
- Reducing the period of Medicare non-billing for which a provider or supplier can be deactivated under § 424.540(a)(1) from 12 months to 6 months.
- Strengthening the program integrity safeguards associated with a provisional period of enhanced oversight under section 1866(j)(3) of the Social Security Act.
Please note that the comment period for the proposed CY2024 Home Health Rule is open until 08/29/2023.

Provider Preview Reports for the October 2023 Refresh
![]()
Please note that the October 2023 refresh will add a new claims-based measure for public reporting:
- Potentially Preventable Hospitalizations (PPH)
The refresh will also remove an OASIS measure from public reporting:
- Drug education on all medications provided to patient/caregiver
Providers have 30 days (until August 16, 2023) to review their performance data. Only updates/corrections to the underlying assessment data before the final data submission deadline will be reflected in the publicly reported data on Care Compare. Updates submitted after the final data submission deadline will not be reflected in the Provider Preview Reports or on the Care Compare website. However, providers can request Centers for Medicare & Medicaid Services (CMS) review of their data during the preview period if they believe the quality measure scores that are displayed within their Preview Reports are inaccurate.
Educational Opportunities

A) New Resource Available: BIMS Video Tutorial
The Centers for Medicare & Medicaid Services (CMS) is releasing a video tutorial to assist providers with guidance application and interview strategies for the cognitive assessment known as the Brief Interview for Mental Status (BIMS). This video tutorial is approximately 20 minutes in length and is designed to provide targeted guidance for accurate coding using live-action patient/resident scenarios. To access the video, click on the following link: BIMS Video Tutorial.
B) CMS Home Health Value Based Purchasing Webinar
The Centers for Medicare & Medicaid Services (CMS) is hosting a Home Health Value Based Purchasing (HHVBP) model webinar on July 27, 2023 at 2-3PM ET.
Overview of the Interim Performance Report (IPR): The July 2023 IPR
During this live event members of HHVBP Model Technical Assistance (TA) Team will provide an overview of the data and information available in the IPR, which will help home health agencies monitor their performance during the calendar year (CY) 2023 performance year.
Note: Only home health agencies with a Medicare-certification date prior to January 1, 2022 will receive a July 2023 IPR.)
C) Home Health and Hospice MAC Collaborative Summit
The 2023 Home Health & Hospice MAC Collaborative Summit: Perfecting Performance By Breaking Down Barriers is now open for registration! This event is being held live, in-person at the Flamingo Las Vegas Hotel & Casino in Las Vegas, Nevada, September 13, 14 & 15.
National Government Services, Inc. (NGS), Palmetto GBA and CGS Administrators have designed this unique collaborative educational opportunity for Home Health and Hospice providers from every state and Medicare jurisdiction.
D) Educational Resource:
Please take a moment and review the following information provided to us by CGS – Home Health and Hospice Billing When a New Medicare Beneficiary Identifier (MBI) is Assigned (cgsmedicare.com).
According to CGS, the questions about this topic have been on the uptick, so we wanted to share this with you.
COLORADO NEWS
ColoradoPAR Program Vendor has a New Name

Please note that Kepro is now Acentra. Acentra Health was founded when CNSI merged with Kepro® in December 2022. Visit the Acentra website https://acentra.com to learn more about the combined companies.
![]()
The CNSI and Kepro merger, and subsequent name change, will not impact the Department’s contract with Kepro or have any impacts to providers or the prior authorization submission and review process.
The only change providers may see is to email signatures, training materials and other Kepro-branded materials as they are transitioned to the new name, brand logo and website link.
You may contact Acentra (formerly Kepro) Provider Relations at COproviderissue@kepro.com or Acentra Customer Service at (720) 689-6340 with questions. Visit the ColoradoPAR: Health First Colorado Prior Authorization Request Program web page https://hcpf.colorado.gov/par to stay informed of any changes or updates.
Attention Colorado HCBS Providers and Direct Care Workers!

Amity Healthcare Group is offering free specialized dementia training courses for Colorado HCBS providers/direct care workers.
![]()
Providers will be able to select from the following courses:
- The Alzheimer’s and Dementia Caregiving at Home (available on Mondays and Wednesdays)
- Creating Safe Home Environment for People Living with Dementia and Alzheimer’s Disease (available on Fridays)
Amity’s newsletters will be archived on Amity’s Healthcare Group website at https://amityhealthcaregroup.
Please do not hesitate to reach out for any assistance or questions via email, phone, or website at https://amityhealthcaregroup.
If you wish to forward this email to your colleague or friend, please feel free to do so. If you received this message as a forward, we invite you to subscribe to our communications at https://amityhealthcaregroup.
Thank you,
Irina Gorovaya, RN BSN, MBA
Amity Healthcare Group, LLC
Home Health Consulting, Education and Outsourcing Services
720-353-7249 (cell) 303-690-2749 (office) 720-398-6200 (fax)
www.amityhealthcaregroup.com







Confidentiality Notice:
The information contained in this message is privileged and confidential information intended for the use of the individual or entity named above.Copyright © 2022 Amity Healthcare Group, All rights reserved.
You are receiving this email because you opted in at our website
Amity Healthcare Group
5600 S. Quebec St Suite 310-A
Greewood Village, CO 8011




























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}